a. Purposes.
(1) Prevent nosocomial infection.
(2) Maintain safe, clean environment for patients.
(3) Provide safety for health care workers.
(4) Prevent cross-contamination of patients or the spread of microorganisms.
b. Scope of Responsibility.
Teaching patients and visitors about procedures and appropriate times for handwashing is an important role for the health care provider. This enables the patient and family to inhibit the spread of microorganisms when health care is continued at home.
The importance of handwashing before and after handling food, after handling contaminated articles, and before and after elimination should be stressed in the teaching process.
c. The Two-Minute Handwash.
A two-minute handwash will provide appropriate protection before you begin working with a patient. A 30-second handwash should be sufficient before caring for another patient. A one-minute handwash should be appropriate if you have handled organic material or a contaminated object.
d. Additional Actions.
In addition to handwashing, other actions can be taken to reduce the chance of transmitting microorganisms. The patient should receive a personal set of care articles, such as a bedpan, urinal, bath basin, thermometer, water pitcher, and drinking glass to prevent cross-contamination. Articles such as contaminated equipment and soiled linen should be placed in special waste containers or laundry bag, and kept away from your uniform.
e. Schedule for Handwashing.
Handwashing is essential:
(1) Before and after caring for a patient.
(2) After contact with organic material, such as feces, wound drainage, and mucous.
(3) In preparation for an invasive procedure such as suctioning, catheterization, or injections.
(4) Before performing a dressing change or contact with an open wound.
(5) Before preparing and administering medications.
(6) After removing disposable gloves or handling contaminated equipment.
STEPS FOR PERFORMING THE TWO-MINUTE HANDWASHING
a. Step One.
(1) Inspect hands, observing for visible dirt, breaks, or cuts in the skin and cuticles (figure 5-1).
(2) Determine contamination of hands.
(3) Assess areas around the sink that are contaminated or clean.
(4) Explain to the patient the importance of handwashing.

b. Step Two.
(1) Remove all jewelry (except plain wedding band) and push watch and long sleeves above wrists.
(2) Adjust water to right temperature and force (figure 5-2).

c. Step Three.
(1) Wet hands and wrists under the running water, always keeping hands lower than the elbows.
(2) Lather hands with liquid soap (about one teaspoon).
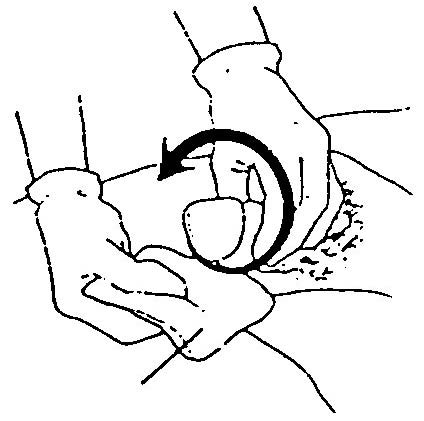
(3) Wash hands thoroughly using a firm circular motion and friction on back of hands, palms, and wrists. Wash each finger individually, paying special attention to areas between fingers and knuckles by interlacing fingers and thumbs, and moving fingers back and forth.
(4) Wash one minute, rinse thoroughly, relather, and wash another minute, using a continuous amount of friction.
(5) Rinse wrists and hands completely, keeping hands lower than elbows (figure 5-3).

d. Step Four.
(1) Clean the fingernails carefully under running water, using fingernails of other hand or blunt end of an orange stick.
(2) Dry hands thoroughly with paper towels. Start by patting the fingertips, hands, and then wrists, and forearms.
(3) Turn off faucets with a dry paper towel (figure 5-4).
(4) Use hand lotion if desired.
(5) Inspect hands and nails for cleanliness.